
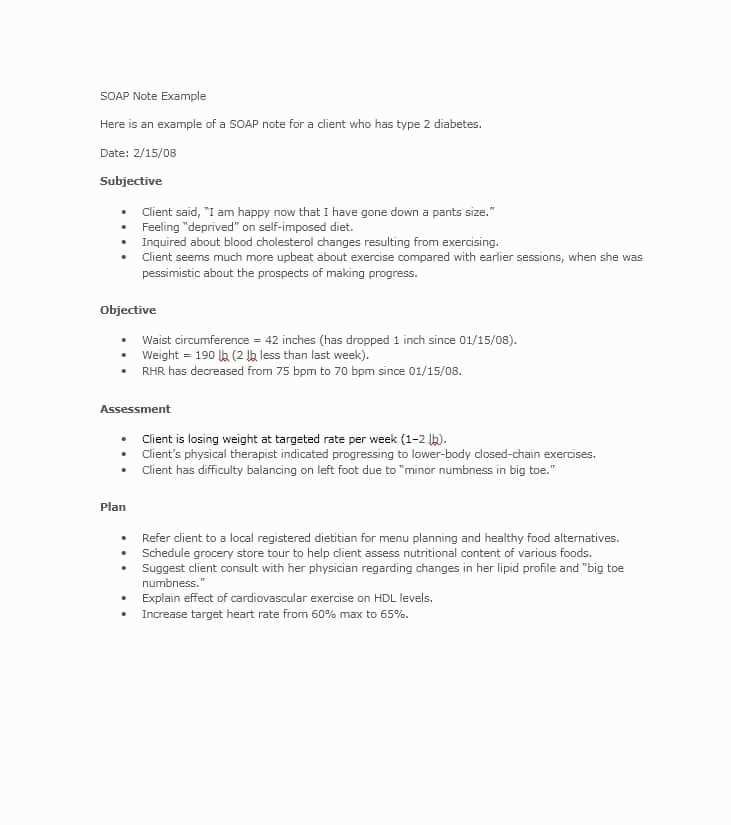
A soap note physical exam refers to a method used by healthcare providers to document the clinical encounter with a patient. It stands for Subjective, Objective, Assessment, and Plan, and serves as a structured format for recording information obtained during a physical examination. This type of documentation is crucial for maintaining accurate medical records and ensuring continuity of care for patients.
The subjective section of the soap note physical exam includes information provided by the patient regarding their symptoms, concerns, and medical history. This section allows the healthcare provider to gather information about the patient’s chief complaint, duration and severity of symptoms, relevant past medical history, and any factors that may exacerbate or alleviate the symptoms.
The objective section of the soap note physical exam focuses on the healthcare provider’s observations, measurements, and findings during the physical examination. This includes vital signs such as blood pressure, heart rate, and temperature, as well as a comprehensive examination of various body systems, such as the respiratory, cardiovascular, gastrointestinal, and musculoskeletal systems. This section provides objective data that can be used to inform the assessment and plan for the patient.
The assessment section of the soap note physical exam involves the healthcare provider’s analysis and interpretation of the subjective and objective data. This is where a diagnosis may be made, or a differential diagnosis considered. The assessment helps guide the healthcare provider in developing a plan for further investigation or treatment.
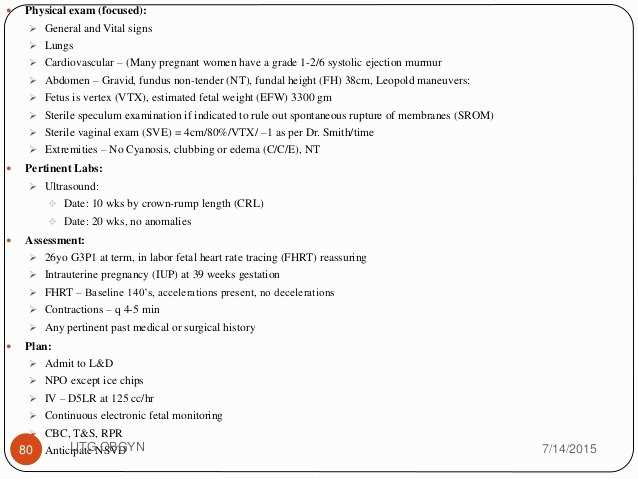
The plan section of the soap note physical exam outlines the recommended course of action for the patient. This may include further diagnostic tests, referral to a specialist, prescription of medication, or lifestyle modifications. The plan is communicated to the patient to provide clarity on next steps and to ensure coordinated and effective care.
Importance of SOAP note in physical exam
SOAP note, which stands for Subjective, Objective, Assessment, and Plan, is a crucial documentation method used in physical exams. It provides a systematic approach to record the patient’s information, findings, assessment, and plans for further treatment.
In the subjective section of the SOAP note, the healthcare provider includes the patient’s complaints, symptoms, and medical history. This information is vital as it helps the provider understand the patient’s condition and determine the appropriate examination and treatment plan.
In the objective section, the provider includes the results of the physical examination, such as vital signs, observations, and any laboratory or imaging findings. This objective data helps in providing an accurate diagnosis and monitoring the patient’s progress over time.
The assessment section allows the healthcare provider to summarize their interpretation of the subjective and objective information. It may include a differential diagnosis or a working diagnosis based on the findings. This section helps in communicating the provider’s clinical reasoning and thought process to other healthcare professionals involved in the patient’s care.
The plan section outlines the course of action that the healthcare provider intends to take for the patient’s treatment. It may include prescribing medications, ordering further diagnostic tests, recommending lifestyle changes, or referring the patient to a specialist. The plan section ensures continuity of care and helps in monitoring the effectiveness of the chosen treatment plan.
The SOAP note serves as a comprehensive and organized record of the patient’s physical examination. It not only aids in providing quality care but also serves as a legal documentation in case of any future references or disputes. Therefore, it is essential for healthcare providers to accurately and thoroughly complete SOAP notes during physical exams.
Organized and standardized documentation
When it comes to medical documentation, organization and standardization are crucial. A SOAP note physical exam is a common method used by healthcare professionals to document patient encounters in a clear and structured manner. This type of documentation helps ensure that all relevant information is captured and can be easily accessed by other healthcare providers.
One key aspect of organized documentation is the use of standardized templates. These templates typically include sections for subjective information, such as the patient’s chief complaint and medical history, as well as objective data, such as vital signs and physical exam findings. By following a standardized template, healthcare providers can ensure that they are consistently capturing all necessary information and that it is organized in a logical and easily understandable way.
In addition to standardized templates, it is important for healthcare providers to use consistent terminology and abbreviations. This helps to avoid confusion and ensure that information is accurately communicated. For example, using the same abbreviations for vital signs, such as BP for blood pressure, throughout the documentation helps to maintain consistency and clarity.
Another aspect of organized documentation is the use of headings and subheadings to separate different sections of the note. This helps to make the information more digestible and allows other healthcare providers to quickly locate specific information they may be looking for. For example, having a separate section for physical exam findings makes it easier for other providers to review the patient’s overall assessment.
Overall, organized and standardized documentation is essential in healthcare. It helps to ensure that all relevant information is captured and communicated effectively, leading to better patient care and outcomes.
Comprehensive patient information
When conducting a physical examination, it is crucial to gather comprehensive information about the patient’s health history and current condition. This information serves as the foundation for the examination and helps guide the healthcare provider in assessing the patient’s overall well-being.
Patient information includes demographic details such as age, gender, and ethnicity. It also involves gathering information about the patient’s medical history, including past illnesses, surgeries, and chronic conditions. This information provides important context for understanding the patient’s current health status and potential risk factors.
- Social history: In addition to medical information, it is important to inquire about the patient’s lifestyle and social habits. This includes asking about smoking, alcohol consumption, drug use, and sexual practices. Such information can be crucial in assessing the patient’s risk for certain diseases or conditions.
- Family history: Gathering information about the patient’s family history of diseases and conditions can provide valuable insight into any genetic predispositions or inherited conditions that the patient may be at risk for. This information helps guide the healthcare provider in determining appropriate preventive measures and screenings.
- Allergies and medications: It is essential to inquire about any known allergies that the patient may have, as well as any medications they are currently taking. Allergies can influence the choice of medications or treatments, while medications can have potential interactions or side effects that need to be considered.
By obtaining comprehensive patient information, healthcare providers can conduct a more informed physical examination and develop a personalized treatment plan. This approach ensures that the patient’s unique needs and circumstances are taken into account, resulting in more effective and tailored healthcare services.
Effective communication and collaboration
Effective communication and collaboration are essential components for successful healthcare outcomes. In the context of a soap note physical exam, these elements are crucial for ensuring accurate and comprehensive patient assessments.
Clear and concise communication between healthcare providers is essential for sharing information, making decisions, and coordinating care. This can include documenting the patient’s medical history, sharing examination findings, and discussing treatment plans. When all members of the healthcare team are well-informed, they can work together seamlessly to provide the best possible care for the patient.
Collaboration plays a vital role in the soap note physical exam process. It involves healthcare professionals from different disciplines, such as physicians, nurses, and specialists, working together to gather and analyze data, make diagnoses, and develop treatment plans. Collaboration fosters a multidisciplinary approach to patient care, ensuring that all perspectives are considered and that the best course of action is chosen.
Efficient communication and collaboration in the soap note physical exam also extend to the patient. It is crucial for healthcare providers to establish open and transparent communication with the patient, ensuring they understand the purpose of the exam, the findings, and the recommended treatment options. This can help build trust, improve patient compliance, and enhance overall patient satisfaction.
In conclusion, effective communication and collaboration are fundamental in the soap note physical exam process. They facilitate the exchange of information, enable coordinated decision-making, and promote a patient-centered approach to care. By prioritizing these elements, healthcare professionals can deliver high-quality, well-coordinated care to their patients.
Components of a SOAP note physical exam
A physical exam is an essential component of a SOAP note, which stands for Subjective, Objective, Assessment, and Plan. The physical exam portion focuses on the objective findings of a patient’s condition and helps the healthcare provider evaluate their overall health and identify any abnormalities or areas of concern.
1. Inspection: This involves visually examining the patient’s body and looking for any signs of abnormalities, such as swelling, bruising, scars, or rashes. The healthcare provider may also observe the patient’s posture, gait, and overall appearance for any signs of distress or discomfort.
2. Palpation: Palpation involves using the hands and fingers to feel different areas of the patient’s body. This can help the healthcare provider assess the texture, temperature, and consistency of the skin, muscles, and organs. They may also check for tenderness, lumps, or other abnormalities that can provide important diagnostic information.
3. Percussion: Percussion involves tapping or striking different areas of the patient’s body to assess the underlying structures and evaluate for abnormalities. The healthcare provider listens for the sound produced and can determine if there is fluid or air accumulation in certain areas, such as the lungs or abdomen.
4. Auscultation: Auscultation involves using a stethoscope to listen to the patient’s internal organs, such as the heart, lungs, and abdomen. The healthcare provider listens for any abnormal sounds, such as murmurs, wheezing, or bowel sounds, which can indicate underlying conditions or issues.
5. Range of motion: Range of motion testing assesses the patient’s ability to move their joints and muscles freely. The healthcare provider may ask the patient to perform specific movements, such as bending or extending their limbs, to evaluate their flexibility and identify any limitations or pain.
6. Neurological examination: A neurological examination assesses the patient’s nervous system, including their reflexes, coordination, strength, and sensation. The healthcare provider may use tools, such as a reflex hammer, to test these functions and identify any abnormalities.
7. Special tests: Depending on the patient’s symptoms or suspected condition, the healthcare provider may perform additional special tests. These can include imaging studies, blood tests, or specific diagnostic procedures tailored to the patient’s individual needs.
- Overall, the physical exam component of a SOAP note plays a crucial role in gathering objective data about a patient’s health and can help guide the healthcare provider in formulating an accurate assessment and developing an appropriate treatment plan.
Subjective Information
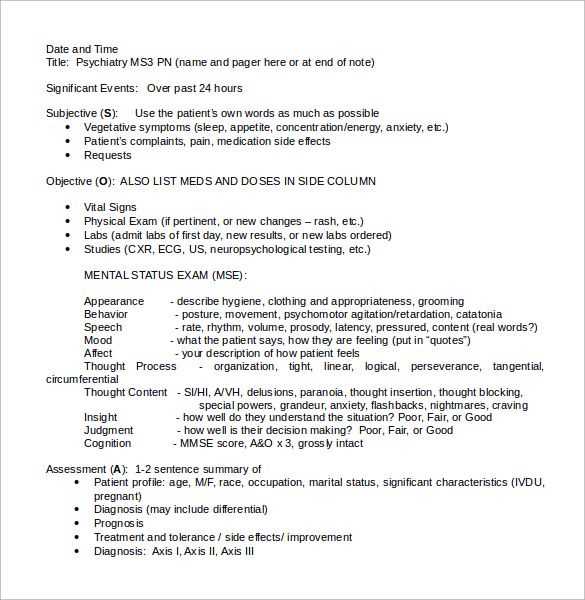
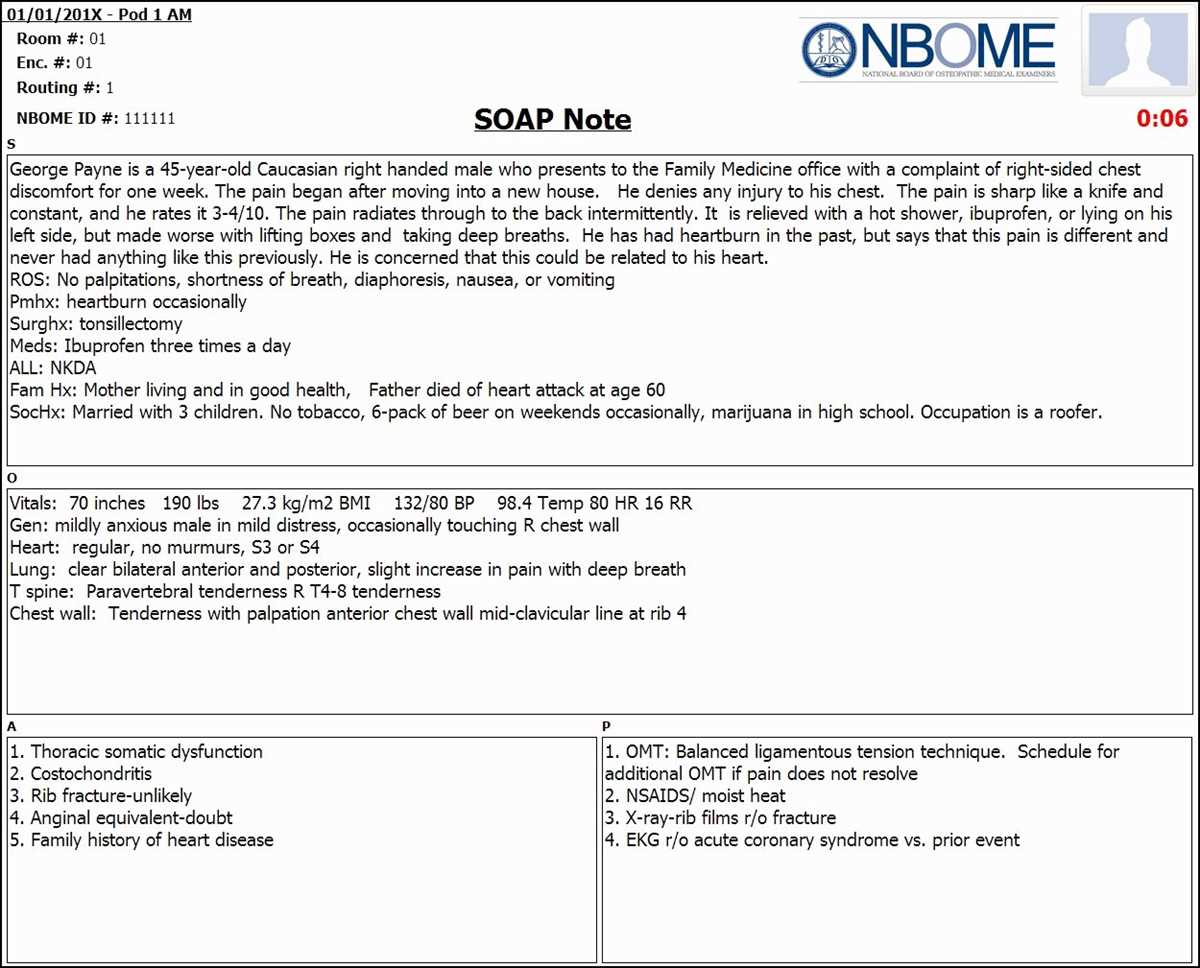
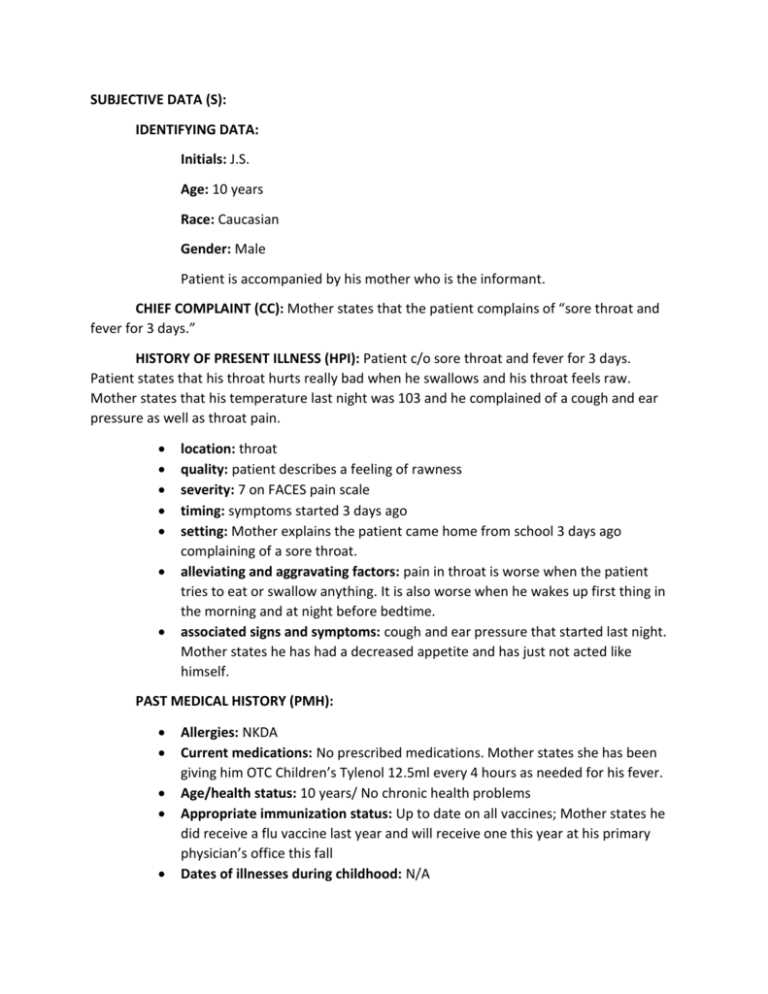
The subjective information section of the SOAP note is where the healthcare provider documents the patient’s personal account of their symptoms and medical history. This information is crucial for understanding the patient’s perspective and providing appropriate care.
During the physical exam, the healthcare provider will ask the patient about their chief complaint, which is the main reason for their visit. The provider will gather information about the onset, duration, location, and severity of the symptoms. They will also inquire about any factors that exacerbate or alleviate the symptoms.
The provider will also ask about the patient’s medical history, including any pre-existing conditions, previous surgeries, medications, and allergies. It is important to gather information about the patient’s family history as well, as certain conditions may have a genetic component.
In addition to gathering information about the patient’s chief complaint and medical history, the provider will also ask about the patient’s lifestyle factors, such as exercise habits, diet, tobacco and alcohol use, and any recent changes in their life or stressors that may contribute to their symptoms.
This subjective information helps the healthcare provider develop a holistic understanding of the patient’s health and formulate an appropriate treatment plan. It is important for the patient to provide accurate and detailed information to ensure the best possible care.
Objective information
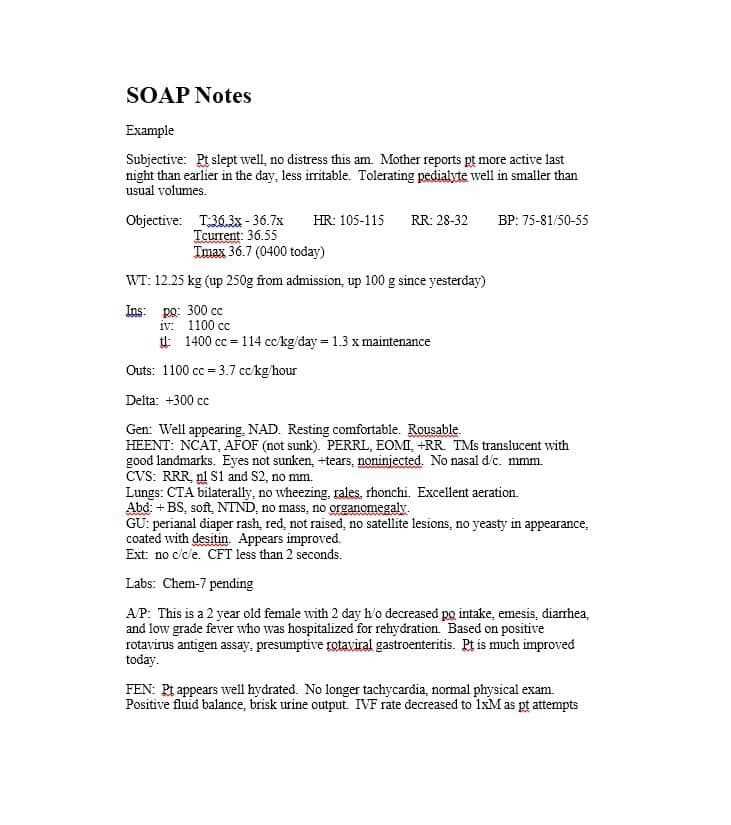
The objective information section of the SOAP note provides specific details about the patient’s physical examination. This includes the healthcare provider’s observations, measurements, and findings from the examination. It is important to document these objective details accurately and objectively, as they provide essential information for diagnosis and treatment.
During the physical exam, the healthcare provider will assess various aspects of the patient’s health, including vital signs, general appearance, and specific body systems. Vital signs such as blood pressure, heart rate, respiratory rate, and temperature are recorded to monitor the patient’s overall health status.
- General appearance: The healthcare provider will note the patient’s general appearance, including factors such as age, race, body habitus, and level of distress. They may also observe for signs of illness, such as pallor, diaphoresis, or altered consciousness.
- Cardiovascular system: The provider will assess the patient’s heart and circulatory system. They will listen to the heart sounds using a stethoscope, palpate the pulses, and inspect for any signs of edema or abnormal fluid retention.
- Respiratory system: The provider will listen to the patient’s lung sounds by auscultation and assess their breathing pattern. They may also measure the patient’s oxygen saturation levels using a pulse oximeter.
- Gastrointestinal system: The provider will palpate the patient’s abdomen, noting any tenderness, masses, or organ enlargement. They will also listen to bowel sounds and assess for any abnormal findings.
- Musculoskeletal system: The provider will assess the patient’s musculoskeletal system, including any areas of pain, range of motion limitations, or deformities. They may also perform specific tests to evaluate muscle strength and joint stability.
- Neurological system: The healthcare provider will assess the patient’s neurological function by evaluating their mental status, cranial nerve function, motor strength, coordination, and sensory perception. They may also perform reflex tests.
By documenting these objective findings, the healthcare provider can provide a comprehensive picture of the patient’s physical examination and assist in making an accurate diagnosis and developing an appropriate treatment plan.